
Equine Gastric Ulcer Syndrome

Updated:
May 13, 2022By Fernando J. Marqués, DVM, Diplomate ACVIM - Associate Professor of Large Animal Internal Medicine - Equine Health Research Fund, Chair - Western College of Veterinary Medicine - University of Saskatchewan
If you’ve ever had a gastric ulcer, you’re familiar with the burning or gnawing feeling in your stomach area that is typical of peptic ulceration of the stomach lining. This pain may last for anywhere from half an hour to four hours, and can occur after eating or even during the night, disrupting sleep. Nobody wants to live with pain or discomfort, and the average person would not hesitate to seek treatment for gastric ulcers. That being said, it is interesting and worth noting that, generally speaking, you would never know that a person has gastric ulcers just by observing their attitude or professional performance.
But what happens with horses afflicted by Equine Gastric Ulcer Syndrome (EGUS)? How do they show us that they are suffering? What causes their gastric ulcers in the first place? And how can we ease their discomfort and prevent its recurrence? These are all questions that warrant further discussion.
Prevalence of Gastric Ulcers in Horses
In a recent study, “The Prevalence and Risk Factors of Esophageal and Non-glandular Gastric Lesions in Thoroughbred Racehorses in Saskatchewan,” conducted at Marquis Downs racetrack in Saskatoon, Saskatchewan, by Marqués F., Epp T., Wilson D., et al., 94 Thoroughbred racehorses in active training were assessed by gastroscopic examination during two racing seasons. Out of the 94 horses, 79 (84 percent) had non-glandular squamous gastric lesions, 70 (74.5 percent) had gastric ulcers, and 9 (9.6 percent) had hyperkeratosis (abnormal thickening of the stomach lining) and/or hyperemia (increased blood supply to a specific area of the stomach lining). None of the horses had esophageal lesions. Interestingly, 34 (48.9 percent) of the 94 horses had won at least one race, and 46 (36.1 percent) had finished in second place during the two-month period prior to gastroscopic examination.
The incidence of gastric lesions in non-racing horses, although variable, is also quite high. Around 58 percent of active show horses have gastric ulcers, and approximately 67 percent of endurance horses, 40 percent of Western performance horses, 67 percent of pregnant Thoroughbred broodmares, and 77 percent of non-pregnant broodmares also have gastric ulcers.

The Equine Stomach
The Equine Stomach and Ulcer Formation
In relation to its size and overall feed consumption, the horse has a relatively small stomach that consists of two distinct regions. The proximal portion of the stomach is the gastric squamous mucosa (also called the non-glandular or esophageal region). The distal portion of the stomach is the glandular region, and contains glands that secrete, among other things, the hydrochloric acid and pepsin necessary for digestion. The non-glandular and glandular regions are divided by a stepped edge called the margo plicatus.
Gastric lesions, including inflammation, erosion, and ulcers, can occur in any region of the stomach, although the clinical syndromes and pathophysiological mechanisms vary according to region. Accordingly, the term Equine Gastric Ulcer Syndrome (EGUS) is used to describe a variety of different conditions, including gastro-duodenal ulcer disease (most commonly seen in foals), glandular gastric lesions related to the administration of non-steroidal anti-inflammatory drugs (NSAID’s), and training-related non-glandular squamous disease.

Healthy epithelium in the non-glandular and glandular gastric regions. Photo courtesy of Dr. Fernando J. Marqués

Gastric ulcers in the non-glandular gastric region. Photo courtesy of Dr. Fernando J. Marqués
Related: The Best Time to Feed Your Horse Before Competition
Causes of Gastric Ulcers
Gastric ulcers form when there is an imbalance between the factors that incite erosion and the factors that protect the stomach. The most common inciting factor is hydrochloric acid, although bile acids, volatile fatty acids, and pepsin may also contribute to disease development. Excessive acid exposure is the chief mechanism of non-glandular squamous disease. The specific protective mechanisms vary among regions of the stomach, i.e. the glandular and non-glandular regions.
Some external factors that can upset the balance between gastric erosion and protective mechanisms are:
- Diet & Feeding Schedule: A high-concentrate, low-roughage diet and intermittent feeding are factors that increase the risk of a horse developing gastric erosion. Because the horse is a natural grazer designed to eat around the clock, the horse’s stomach, as part of the normal digestive process, secretes hydrochloric acid regardless of whether the horse is actually eating. Feed material in the stomach acts as a buffer (a substance capable of neutralizing the acid, thereby maintaining normal acidity), minimizing potential deleterious effects of the acid. If a horse is only fed twice a day, there are prolonged periods when the stomach is empty, thus leaving the stomach more susceptible to acid injury.
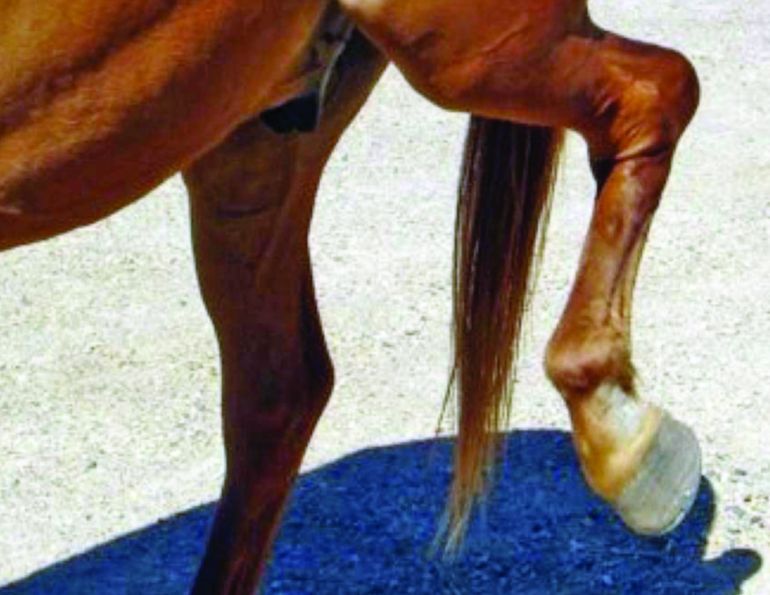
- Exercise Intensity: A study conducted by Orsini J., Hackett E., et al revealed that the prevalence and severity of training-related non-glandular squamous disease increase with the duration and intensity of training. A second study (Lorenzo-Figueras and Merritt), in 2002, demonstrated that during exercise the horse’s stomach is compressed by the abdominal viscera and diaphragm, forcing acidic contents proximally (upward) and inducing acid-mediated injury to the non-glandular squamous mucosa. Horse owners, riders, and trainers need to be aware that increasing training intensity can predispose horses to gastric ulcer formation.
- Illness: The prevalence of gastric ulcers in critically ill foals is higher than in normal foals, and it is possible that the physiologic stress associated with illness causes ulcer development.
Diagnosis
While a horse’s history and a description of clinical signs are important in diagnosing gastric lesions including ulcers, veterinarians rely on an endoscopic examination (gastroscopy) to make a definitive diagnosis. Prior to the examination, the horse is usually fasted for eight to ten hours, and denied access to water for one hour. The procedure itself, for which the horse is sedated, consists of passing a three-metre, flexible videogastroscope through the nasal passage of the horse into the stomach (same as passing a nasogastric tube).

An estimated 60 to 90 percent of racehorses in active training suffer from gastric ulcers. The prevalence of gastric lesions in non-racing horses, although variable, is also quite high, with around 58 percent of active show horses suffering from gastric ulcers.
The stomach is insufflated with air and distended until the glandular and non-glandular regions can be observed. A systematic approach for assessing the stomach and duodenum (first portion the intestine exiting the stomach) is used. When the gastroscopic examination is completed, the air from the stomach is removed using a suction pump. Most practitioners use a grading system that was developed by the Equine Gastric Ulcer Council to classify the gastric lesions in the non-glandular portion of the stomach: the system ranges from Grade 0 (normal) to Grade 4 (severe ulceration).
Clinical Signs
Clinical signs of EGUS often vary according to cause, location, and severity of the gastric ulceration, and age and general wellness of the horse.
- Adult horses: The most common clinical signs of gastric ulcers include low-grade colic, poor body condition, and decreased performance, but these can vary; some adult horses with endoscopic evidence of gastric ulcers may show no signs or very subtle symptoms. Most gastric lesions in adult horses are found in the non-glandular squamous mucosa, especially adjacent to the margo plicatus, but lesions in the glandular region around the pylorus (opening from the stomach into the duodenum of the small intestine) are not uncommon.
- Neonatal foals: With gastric ulceration, neonatal foals may suffer from colic and diarrhea, grind their teeth or salivate continuously, have little or no appetite, and tend to lie on their backs. Since very few foals with endoscopic evidence of gastric lesions show symptoms, if any of these clinical signs are observed, chances are the ulceration is severe. As in adult horses, the majority of gastric lesions in young foals are found in the non-glandular squamous mucosa. However, physiologic stress associated with illness has been linked to gastric ulcers in neonatal foals, and these lesions are typically found in the glandular epithelium.

The prevalence of gastric ulcers in critically ill foals is higher than in normal foals, indicating that the physiologic stress associated with illness may cause gastric erosion.
Older foals: Clinical signs like diarrhea, poor appetite, poor growth, and poor body condition in older foals are associated with severe non-glandular squamous epithelial lesions. The clinical signs in foals with duodenal ulceration are similar to those associated with gastric ulceration, and include colic, teeth grinding, continuous salivation, and diarrhea. These foals may also suffer from delayed emptying of their stomachs and gastroesophageal reflux.
Related: Equine Colic - Signs, Symptoms, Treatment
Treatment
Since excess acid exposure is the main reason behind squamous mucosal erosion and ulceration, most veterinarians turn to anti-ulcer therapies with the aim of suppressing or neutralizing gastric acid.
- H2 antagonists, such as ranitidine (Zantac®) or famotidine (Pepcid®), can successfully raise the gastric pH and resolve gastric ulcers in foals and adult horses. However, the degree and duration of acid suppression by H2 antagonists varies from horse to horse. Practitioners routinely administer anti-ulcer drugs to critically ill neonatal foals as a prophylactic measure, but its effectiveness remains controversial. Treatment responses vary and there’s also a concern that the use of prophylactic anti-ulcer therapy may suppress the function of gastric acidity in preventing bacterial translocation in neonatal foals. The acidic environment in the foal’s stomach is one of the normal protective barriers against potential invading microorganisms.
- Proton pump inhibitors, such as omeprazole (available under the trade name Gastrogard®) have been effective in healing naturally-occurring cases of gastric lesions. Several research studies show that omeprazole is effective in reducing or eliminating the severity of gastric ulcers in Thoroughbred racehorses undergoing intensive training. Omeprazole is considered the “gold standard” for treating and preventing gastric lesions in horses. It is important to note that there are some compounded omeprazole products, which are generally cheaper than the commercial products. The Canadian Veterinary Medical Association states in its “Guidelines for the legitimate use of compounded drugs in veterinary practice (2006)” that “compounded drugs are unapproved drugs that have not undergone the Health Canada approval process.” These compounded products have not been evaluated by Health Canada for safety, stability, potency, efficacy, and consistency of manufacturing, therefore only commercial products approved by Health Canada, such as Gastrogard®, are recommended for the treatment and prevention of gastric ulcers.
- Sucralfate (Carafate®) is effective in treating peptic ulcers in humans, but its efficacy in treating ulcers in the equine gastric squamous mucosa is unknown. Sucralfate may be effective for treating stress-induced ulcers in neonatal foals, but so far, there is no clinical evidence to support this theory.
- Antacids, such as Maalox®, can reduce gastric acidity in horses, but their effects are short-lived (lasting approximately two hours) and require large doses several times a day.
- Prokinetics can be part of a therapy plan when veterinarians suspect delayed gastric emptying without any physical obstruction in a patient. This treatment is also useful in treating foals with duodenal disease and gastroesophageal reflux.
Horses are designed to graze around the clock, and a horse’s stomach continues to secrete hydrochloric acid regardless of whether he is actually eating.
To treat or not to treat?
Many veterinarians and owners argue the need for treatment of gastric lesions in horses. However, the fact that such a high percentage of horses (up to 90 percent of Thoroughbred racehorses in training) have gastric lesions, and that most of these horses with gastric lesions do not show clinical signs, might lead others to believe that EGUS is not something to worry about. Nevertheless, no one would dispute that a horse with gastric lesions and showing clinical signs should be treated. So, the question becomes, should a horse with gastric ulcers that is not showing clinical signs (asymptomatic) be treated?
For the same reason that a person with gastric ulcers would not hesitate to start treatment, the decision to treat a horse with similar gastric lesions should not be distinct. If a person can have gastric ulcers without exhibiting signs of pain and discomfort that are evident to others, why should we assume that the horse with gastric lesions that demonstrates no clinical signs is not also suffering the same pain and discomfort? And, how accurate are our tools to assess mild pain and discomfort in the horse? Do we wait until our horse is sweating, colicky, and rolling to take action? The answer is no. Minimizing pain and discomfort in horses is part of the welfare every horse deserves and what we all want for them.
Related: How to Protect Your Horse from Ulcers
Main photo: During strenuous exercise, horse’s stomach is compressed, forcing acidic contents upward. Horse owners should be aware that increasing training intensity can increase horse’s risk of developing gastric ulcers. Credit: John Harwood/Flickr
Acknowledgment: I would like to thank Mrs. Monique Cardalda for her help in preparing this article.

Blogs & Podcasts

Advertisement

Related Articles






Advertisement

Featured Stories









Advertisement
