The High Risk Mare

Updated:
February 18, 2021By Juan C. Samper DVM, MSc., PhD Diplomate ACT and Tracy A. Plough DVM
Waiting for the birth of a foal seems to take an eternity, but the day when your newborn foal will stand beside its dam and nurse for the first time is almost here. Most mares will foal without problems, but if you have a high risk mare you should alert your veterinarian of potential problems early, and monitor her closely during her pregnancy to protect your emotional and financial investment.
What constitutes a high risk mare? Typically, mares with a known history of reproductive disease, or trouble maintaining pregnancy or delivering live foals, are collectively referred to as “high risk mares.” Some of these mares have acquired an infectious disease during pregnancy, others appear healthy but habitually have weak or sick foals.
Early Introduction to the Foaling Environment
Mares should be introduced into the foaling environment one month before foaling. Doing so will minimize stress on the mare by allowing her to acclimatize to the environment, and will expose her system to the pathogens in the area which will stimulate her immune system to produce antibodies. Booster vaccination of pregnant mares against common pathogens should be performed one month prior to foaling.
It is important that the foaling environment be as clean as possible to avoid a potential buildup of pathogens. Foals that receive an adequate, timely amount of colostrum can still succumb to infection if the pathogen burden is very high in the environment.
The foaling stall should be a minimum of four metres by four metres, in a quiet location, and have good bedding and footing, a water bucket off the floor, and removable feed tubs.
Providing the weather is mild, foaling outside in a sunny, grassy paddock or pasture is an acceptable practice. However, foaling outdoors carries additional risks as it makes careful monitoring more difficult, other mares may try to steal the newborn foal, fetal membranes may be lost or carried off by scavengers, and foals may drown or be injured in fences. In addition, cold and wet foals may become hypothermic and will not absorb colostrum as well or be as vigorous as foals born in milder weather, as they will have to expend more calories for heat than for locomotion.
Prefoaling Mammary Secretion Testing
Fortunately, ninety percent of all foalings occur without any intervention needed. However, the other ten percent often result in problems where the lives of the mare and/or the foal are at risk. Methods used to detect changes in mammary secretion are beneficial for farm managers because these tests indicate when a mare needs to be watched closely for parturition. The use of breeding dates and mammary development are unreliable predictors of parturition in the horse because of the variability (320 to 365 days) in normal gestational length. Changes in the composition of the prefoaling mammary secretion are used to determine fetal maturity and readiness for birth. There are many test kits available that detect increases in total calcium ions or calcium and magnesium ions. Calcium ions increase dramatically in the prefoaling mammary secretion within a few days prior to parturition. This increase is used to indicate impending parturition, the safe time window for induction of parturition, and to predict the outcome in cases of premature delivery. One of the advantages of using these kits is that a specimen can be drawn daily or twice daily, so that the mare can be handled and watched closely during this time. This allows managers to detect problems with their pregnant mares that they may otherwise have missed. The kits are better predictors of when the mare is not going to foal than when she is going to foal, hence farm managers and owners have a better idea of when a mare should be watched closely. Mares with low levels of calcium are highly unlikely to foal, while mares at or above the kit’s threshold value are ready to foal and likely to foal within 48 hours of first reaching the kit’s reported threshold level of calcium.
Prefoaling mammary secretion may also be tested for immunoglobulin content through the use of a colostrometer or a test kit. A mare with poor quality colostrum may have a foal at risk of failure of passive transfer. In one study, mares older than 15 years of age were shown to have a tendency to have colostrum with lower specific gravity than younger mares. Foals from dams with poor quality colostrum may be supplemented with colostrum from another mare, or tested for systemic immunoglobulin levels after 12 hours. It is preferable to cross match the foal’s blood against the mare’s colostrum to remove the risk of neonatal isoerythrolysis (NI) from an incompatible donor. Neonatal isoerythrolysis is a disease in foals whereby the antibodies in the colostrum recognize and adhere to foal’s red blood cells. These red blood cell/antibody complexes are then destroyed by the foal, and the foal develops a life threatening immune mediated anemia. The risk of acquiring NI from a donor is quite low and only a low percentage of mares with blood group risk develop red blood cell sensitization, thus many managers will use unmatched colostrum if there is no history of NI in the mare. Conversely, mares with a history of having a foal with NI may benefit by testing for blood group compatibility prior to mating to choose a compatible stallion, or the foal should be prevented from nursing and the mare milked for two days following foaling to remove colostrum from the udder, after which the foal may be allowed to nurse the mare. It is recommended that a foal receive at least 1.5 litres of good quality colostrum in the first 24 hours of life. Some colostrum, even from another species such as a cow or goat, is better than no colostrum at all. Oral commercial colostrum supplements are also available, and plasma may be fed orally to foals to provide some protection. Foals may need to be transfused with plasma to achieve passive antibody protection if more than 24 hours has elapsed since birth.
Parturition
Parturition is the process that prepares the foal and dam for birth, initiates the labour and delivery of the foal and placenta, and prepares the mare for the beginning of lactation. In a broader sense, perinatology encompasses parturition and many other aspects of clinical importance. It has been best described by Dr. Peter Rossdale: “Perinatology contains elements which are both maternal and foetal, adult and newborn, in a remarkable example of collaborative biological function that is partly parasitic, partly symbiotic, and partly independent. It involves a wide variety of disciplines and has evolved through direct scientific experimentation and by more clinical observations.”
In spite of remarkable advances in many other areas of equine reproduction, our understanding of perinatology and parturition in the horse still remains unclear. Parturition in the mare is an exciting time, where almost a year’s worth of waiting comes to fruition. Mares are notoriously sneaky at foaling while unobserved, hence many monitoring systems have evolved to determine when a mare is foaling. Closed circuit TVs, baby nursery monitors, contact devices with transponders, electronic tampons such as Birth Alert, and magnets such as Foal Alert have all been used with some success. The disadvantage of these monitoring methods is that the observer must be awake to check the monitor. The transponder methods set off an alarm when the contact is broken or the temperature changes awaken the attendant. These methods sometimes give false alarms, and may not be activated in cases of abnormal or difficult labour. The advent of prefoaling mammary secretion testing has taken many of the long nights and much of the guesswork out of foal watch duty.
The foaling environment should be clean and well lighted. The list of supplies to have on hand for foaling includes halter and lead rope, tail wrap, buckets, soap, cotton, obstetrical ropes or chains with handles, sharp knife or scalpel, towels, and navel treatment solution.
Preparation for parturition in the mare varies from the visually obvious to the visually obscure. Ventral edema (abdominal swelling) is common in late pregnancy and the edema is usually pitting (indentation persists after applied pressure has been released). Exercise will reduce the amount of edema, which is usually of no clinical significance. Occasionally treatment with diuretics may be required, particularly in postpartum mares to allow comfortable movement and to assist with milk let-down. The connective tissue around the tailhead and sacrosciatic ligaments in the normal mare become palpably relaxed the week before parturition. In older mares there may be a visible sinking in the croup region of the mare. The vulva of the mare may also relax, with walls thickening, and the creases or puckers in the top will straighten out typically within 12 hours of delivery. To follow these useful signs the mare should be observed twice daily.
An increase in mammary development usually occurs over the last month of gestation. The secretion of fluid into the udder begins as early as six weeks before foaling, and the secretion itself goes through a series of changes in colour and consistency. The prefoaling mammary secretion goes through ion changes which may be used reliably as a predictor of impending foaling in normal pregnancies. Waxing up, where a small amount of secretion is seen hanging from the teat opening, often occurs within 24 hours of parturition.
Related: Effects of Longer Day Length on Pregnant Mares
The mare has a pattern of hormonal change more like the human, and is quite distinct from the pattern of change in ruminants. Shifting steroid hormone ratios are responsible for the onset of labour through a change in the coupling and efficiency of communication between myometrial cells through structures called connexins or gap junctions.
The first stage of parturition, or stage one of labour, is experienced by the mare as the onset of coordinated uterine contractions. These contractions are usually not manifested outwardly by the mare until she begins to experience obvious discomfort. Stage one presumably takes about 14 hours in mares with the last four hours resulting in the mare sweating, groaning, holding her breath, looking at her flank, swishing her tail, stall walking, restlessness, and dripping or streaming milk. These contractions serve to dilate the cervix, and result in the outward bulging and rupture of the outer placental membrane called the chorioallantois (CA). Presence of the bulging CA or the foal’s feet in the vagina triggers the reflex release of oxytocin and the mare begins to strain. The rupture of the CA releases allantoic fluid, which is yellow, urine-like fluid. Unlike urine, this fluid flows passively out when the mare moves, or gets up and down, and flows actively out as the mare strains.
The rupture of the CA begins the second stage of labour, and the mare’s straining will increase in force and frequency. The second stage of labour may be very brief, ranging from five to thirty minutes. The mare may repeatedly get up and lie down during this time, and may roll in an attempt to assist the foal in attaining the birth posture. Foals are born in the diver’s position with both forelegs extended, followed by the head and neck. One of the forefeet normally appears at the vulva a few minutes after the rupture of the CA. The foal’s second foot is then usually visible about ten centimetres behind the first foot, followed by the muzzle.

Foal’s are born with both forelegs extended, followed by the head and neck. One forefoot usually appears with the second forefoot about ten cm behind, followed by the muzzle. Photo: Pam MacKenzie
The presentation of a red bag or sack at the vulva instead of the bluish opaque amnion constitutes an emergency. The red bag is the CA, which is normally attached to the uterine lining and supplies the foal with oxygen. The presence of this membrane indicates that a premature separation of the placenta is occurring causing asphyxiation of the foal: this tough membrane must be broken. The foal’s feet in the amnion are usually present and the delivery of the foal should be assisted.
In all cases of obstetric assistance, traction on the foal’s limbs should be directed toward the mare’s hocks. Traction should be primarily applied as the mare strains and then the tension reduced as the mare stops straining. The normal presentation of the foal’s head into the vagina usually causes the mare to lie down, and forceful abdominal straining occurs where the mare will lie out flat, with legs straight, and push causing the rapid passage of the foal. The feet, head, chest, and hips will be delivered and mare will stop straining, leaving the foal’s hind feet in her vagina. The amniotic membrane is normally intact during delivery and surrounds the foal.

If assistance is needed, traction should be directed toward the mare’s hocks. Photo: Pam MacKenzie

The foal should free itself of the amniotic membrane as it struggles to sit up. Photo: Pam MacKenzie
Struggling by the foal to sit up should free this membrane from its face, however, if not broken immediately the foaling attendants should tear it free from the foal’s face to avoid suffocation. A normal foal will be able to maintain a sternal position within five minutes of birth; any foal that is not able to sit up in this time frame will usually require assistance, and sometimes intensive care. Asphyxiated foals will often be stained yellow from the passage of meconium prior to delivery. Mares will often remain recumbent and rest for 20 minutes or more following delivery. Struggles by the foal will break its umbilical cord, usually at a natural constriction in the cord near the abdomen. The foal typically initiates contact with its dam.

The foal should maintain a sternal position within five minutes of birth. Photo: Pam MacKenzie
Stage three of labour is the passage of the placenta. Mares typically deliver their placenta thirty minutes to two hours following foaling. The foal should be encouraged to nurse frequently, and if the placenta is not passed within four hours the mare should be treated with oxytocin to effect to stimulate uterine contractions. Sensitivity to oxytocin varies with the individual and with time, hence doses should be chosen with care and tailored to the individual. Uterine exhaustion or excessive stimulation of the uterus can both lead to uterine prolapse. Careful monitoring should accompany treatment. It is advisable to always monitor the temperature of a mare with retained fetal membranes for fever and infection, and treatment with penicillin and anti-inflammatory medication is advisable to minimize the risk of potentially life threatening endotoxemia, septicemia, and laminitis.

Passing the placenta is the third stage of labour. Photo: Pam MacKenzie
Management of the High Risk Mare
A typical sign of trouble in a mare’s pregnancy is precocious or premature lactation. The cause of the early lactation should be ascertained, and the most common causes include twin pregnancy, infectious placentitis, and impending abortion. Prefoaling mammary secretion ion changes may be used as a predictor of fetal maturity and subsequent viability in distressed pregnancies, as fetal maturation accompanies the ion changes in the mammary secretion.
Related: Feeding the Broodmare - Eating for Two
One of the relatively common causes for concern during pregnancy is the sudden, excessive, extreme accumulation of painful edema, which is often accompanied by a characteristic stance of the mare. She will stand with her legs wide and camped out behind, and may be reluctant to move; this may indicate impending rupture of the prepubic tendon. The swollen tissues will be painful, while normal physiologic edema associated with pregnancy is not tender. Ultrasound examination of these tissues may show hemorrhage, edema, muscle fibre disruption, or hematoma formation in the fascial planes of the tissues. The breakdown of the prepubic tendon may cause the mare’s udder to point forward at an abnormal angle. Rupture of the prepubic tendon is a serious condition and commonly results in the death of the mare. The rupture of these tissues may allow the viscera to adhere to the skin resulting in ileus, colic, shock, or death. In such a case, a decision may be required to save the mare or the foal, and the viability of the foal ascertained.
Older mares are more likely to have a prepubic tendon rupture. In milder cases, or following injuries or surgery, a large cotton-elastic support wrap with a dorsal velcro closure may be applied around the mare’s abdomen. Two support wraps may need to be sewn together to accommodate the large abdomen of a pregnant mare. Parturition may be induced to save the life of the mare, or a terminal cesarean section may need to be performed. Other hernias, such as those of the ventral flank, may also occur in association with late pregnancy or parturition. The primary rule-out in these cases is trauma where the mare may have fallen or sustained an injury to her abdomen.
Mares presented with precocious mammary development, labour, vaginal discharge, or fever should receive a full examination which includes the following observations and procedures:
- Review of reproductive history;
- Physical examination and taking of vital signs;
- Observation of posture and gait;
- Checking digital pulse quality;
- Mammary secretion testing;
- Checking extremities for signs of previously dripped milk;
- Abdominocentesis if depressed or feverish;
- Checking for discharge;
- Evaluating perineum;
- Performing a rectal examination to check consistency of cervix and uterus; the position, presentation, posture, and activity level of the fetus; the position of the broad ligaments of the mare; and palpation of all other accessible structures;
- Determining the viability of the fetus: fetal motion, ocular reflex, biophysical profile;
- Performing a vaginal examination.
Sometimes the clinical management of a mare, such as the decision to induce parturition or the decision to perform a surgery on a mare, depends on the condition (stability or viability) of the fetus. The fetal status can be investigated through transrectal and transabdominal ultrasonography. The fetal heart rate, presence of fetal motion, and heart rate accelerations in association with fetal motion provide a fair amount of information regarding the welfare of the fetus. Fetal gestational age and approximate birth weight may also be estimated, and a fetal biophysical profile obtained. An ultrasound examination of the placenta, fetal fluids, and fetal parts, both transrectally and transabdominally, can be performed.
Related: Colostrum - An Exceptional Superfood for Animals and Humans!
The uteroplacental thickness should be measured because the junction of the two tissues is not distinct. Thickening at the uteroplacento-cervical region may indicate an ascending infection. The presence of excess edema and extensive separation of the placenta with exudate intervening between the placenta and uterus is not normal. These findings indicate that a vaginal examination should be performed.
The mare must be cleansed with a mild soap to remove all fecal matter, and then dried off. The vagina should have a good seal, and should be dry and pale if the mare is not close to delivery. The cervix may be cautiously palpated with a gloved hand, and may give some indication if the mare is dilating; however, most mares will have a soft, short cervix in late pregnancy. A tenacious yellow mucous plug may be visible in the cervix. A “bloody show” (a small amount of clear mucus with blood in it) immediately prepartum is an uncommon finding, but is not an abnormality in the mare. However, any purulent or red brown bloody discharge from the cervix or in the vagina is abnormal. A swab of the material should be submitted for cytologic evaluation and culture. A gram stain of discharge material may help indicate what organism is involved.
Some mares may have urine in the vagina, which creates chemical irritation and is considered abnormal. As pneumo-vagina (the involuntary aspiration of air into the vagina) is one of the predisposing factors causing pooling of urine in the anterior vagina, some of these mares may be helped by a Caslick’s surgery (lips of vulva are stitched together), while others require other surgical procedures.
The gestation age of the fetus should be calculated and the expected fetal aortic diameter predicted. A fetus with a smaller-than-calculated orbital (eye) diameter is either a result of a wrong breeding date or is growth retarded. Similarly, a fetus with a small aortic diameter is also likely to be growth retarded and may not be normal at birth. The fetal fluids should appear black, with small particulate matter floating in the fluids. The particulate matter itself is of no concern, however, very dramatic rapid changes in fetal fluid density may be associated with meconium passage in amniotic fluid or infection.
Fetal heart rate or umbilical pulsations may be used as an indicator of fetal viability. Very high or low heart rates are associated with fetal stress or asphyxia. Cardiac arrhythmias are also abnormal in fetuses. The heart rate of the equine fetus decreases with gestational age. The normal heart rate of a fetus at less than 330 days of gestation is about 76 beats per minute; two standard deviations below the mean heart rate, or below about 50 bpm, indicates fetal compromise.
The information obtained from these examinations may assist in determining the progression of a high risk pregnancy. Thus, it may be useful to have some baseline information on the fetus if it is necessary to evaluate the fetus at a later stage of gestation.
There are major limitations in the information available on the ability of antibiotics to reach the placenta. The antibiotic combination most commonly used is trimethoprim sulpha. Penicillin does not readily cross placental tissues into the fetus, and prolonged antibiotic therapy is advised because of the nature of the tissues being treated. Local irrigation with warm saline of the exposed piece of placenta showing at the cervix has been advocated by some veterinarians, to remove debris. Agents to stop preterm labour may be required, and non-steroidal, anti-inflammatory agents may also be suggested. Regular monitoring of the fetus will assist in determining when an induction of labour should be performed.
Mare owners should be cautioned about the potential for an abnormal foal, especially when fetal heart cardiac abnormalities are detected or fetal growth retardation is present, and should carefully consider the costs associated with neonatal intensive care and management of a compromised newborn.
Dr. Juan Samper, MSc, PhD, Diplomat ACT, operated JCS Veterinary Reproductive Services in Langley, BC, from 1993-2017. He has consulted with breeders and veterinarians in over 25 countries. He served as the Associate Dean Clinical Affairs at Ross University School of Veterinary Medicine from 2014 to 2017, and is presently the Associate Dean of Students and the University of Florida College of Veterinary Medicine.
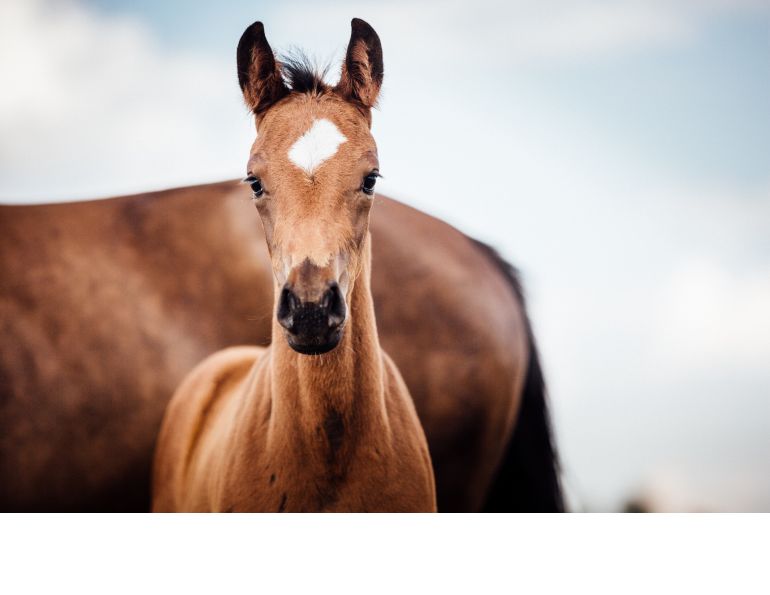
Main Photo: A healthy mare and foal is the goal of every breeder. Credit: Pam MacKenzie Photography

Blogs & Podcasts

Advertisement

Related Articles







Advertisement

Featured Stories









Advertisement
